Hip Dysplasia
Developmental dysplasia of hip is a condition in which part of the hip joint (ball and socket joint) is dysplastic or abnormal. It is usually the socket or acetabulum part of hip joint which is usually not deep or curved enough (flat) to keep the ball (head of femur/thigh bone) concentrically reduced. Depending upon the severity, the ball can be either partially or completely out of the socket. In other cases the hip joint is reduced but is unstable and can be dislocated on clinical manueveres.
Its incidence varies between 1 to 3 in every 1000 live births. It can be present at birth or during the first year of life.It can be present in isolation or in association with other musculoskeletal disorders. It is usally more common in females, first born child, breech presentation (bottom of baby is delivered first in place of head) and in oligohydramions pregnancies.
Every child should be examined thoroughly by a paediatrician to rule out ddh and in case of any doubt, the child should be timely referred to a paediatric orthopaedic surgeon.
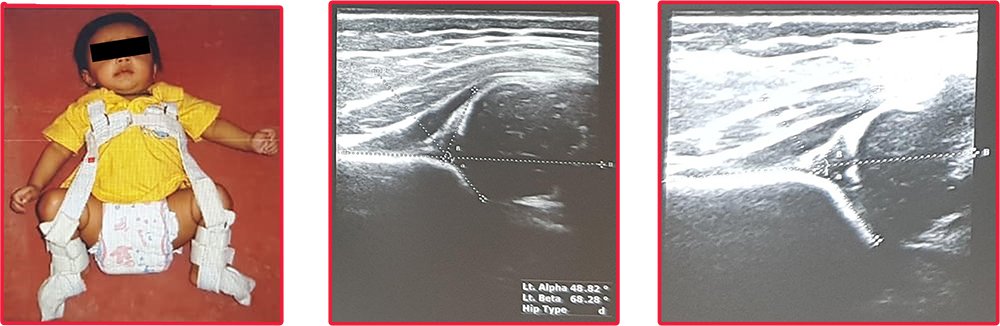
It is sometimes difficult to detect DDH early as there are no obvious signs present. However a careful clinical examination of both the lower limbs will be able to make out a diagnosis. Apart from examination there are other studies including USG and X-rays of the hips to confirm the diagnosis of DDH.
Treatment of DDH is age dependent:
0 to 6 months: Children with DDH in this age group can be managed with soft brace also known as Pavlik harness which keeps the hips in place by flexing and abducting them. This helps in better and more normal development of dysplastic acetabulum.
B6 months to 2 years: A Pavlik harness is not appropriate for this age. A ddh diagnosed in this age needs evaluation under anaesthesia in which arthrogram is done to assess concentric close reduction of hip. If close reduction is achieved, a hip spica cast is applied in appropriate position for 2-3months. If a close reduction doesn’t work, then an open reduction is to be done to attain reduction. If the reduction is too tight, sometimes a thigh bone shortening is also done to prevent pressure on the head and subsequent vascular damage. Also sometimes, a reshaping of the socket is also required by doing an acetabular osteotomy. After the open surgery, a hip spica is applied for 3 months.
Older kids> 2 years: Kids older than 2 years frequently need a open reduction with femoral and pelvic osteotomies.
Outcomes: Regular long term follow ups are required to ensure normal development of the hip joint. Most of children with have good functional hips after appropriate treatment. Some patients may need further surgery for residual dysplasia. However if left untreated, dysplastic hips can lead to early degeneration and pain of the affected hips.
Don’t Let Your Child Suffer! Contact Us Today!
If your child is suffering from any kind of Bone and Joint related problems